
PLLA vs PDLLA vs PLA: Key Differences in Collagen Biostimulators 2026
The PLA Family: Understanding the Basics
Acidum polylacticum, implentores ex PLPLA derivati, sunt polymeri synthetici. Sunt biocompatibiles atque biodegradabiles. Volumen faciei vel corporis restituunt. Collagenum excitant. Sunt variae dispositiones molecularis acidi lactici. Exempla sunt PLLA, PDLA, et PDLLA. Hae dispositiones mores clinicos variant.Volumen faciei vel corporis restituunt et collagenum excitant. Dispositiones molecularis acidi lactici variant. PLLA, PDLA, et PDLLA mores clinicos et usus determinant.usus determinant.

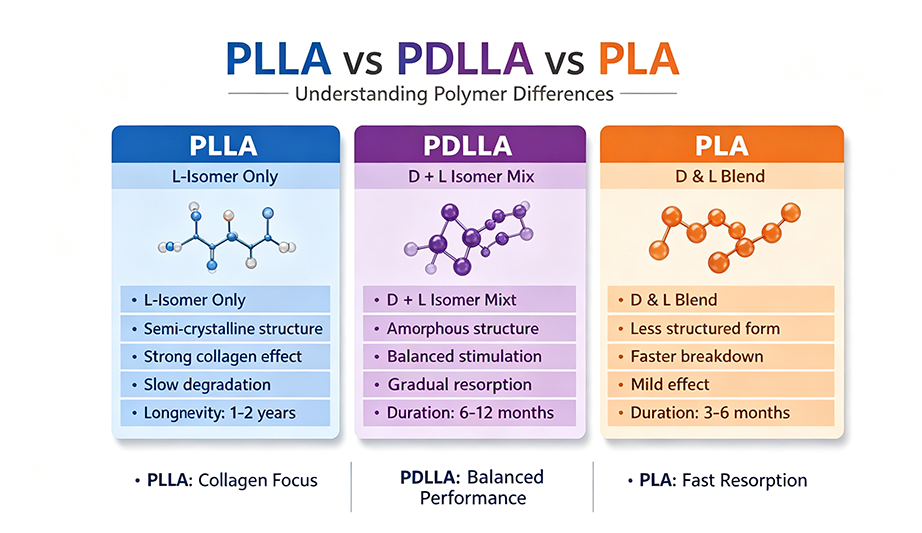
Lactic acid exists as two optical isomers: L-lactic acid and D-lactic acid. When polymerized, these isomers create different forms of polylactic acid. PLLA (Poly-L-lactic acid) consists of all L-isomers, PDLA (Poly-D-lactic acid) consists of all D-isomers, and PDLLA (Poly-DL-lactic acid) is a racemic mixture of both. A 2025 structural-property review published in the International Journal of Nano and Biomaterials confirms that these distinct physicochemical properties "are crucial in initiating subclinical inflammation and activating fibroblasts for collagen production". For practitioners seeking high-quality biostimulatory fillers, Aurothread's PLLA filler collection offers professional-grade products designed for optimal clinical outcomes.
PLLA: The Gold Standard for Collagen Stimulation
PLLA (Poly-L-lactic acid) is the most studied and widely used PLA-based filler in aesthetic medicine. Its semi-crystalline structure, with a glass transition temperature (Tg) of 60-65°C and melting temperature (Tm) of 175°C, gives it significant mechanical strength and durability. According to research published in Biomaterials, PLLA is "usually hard and brittle," which can hinder its use in some medical applications but provides excellent structural support for volume restoration. Importantly, PLLA demonstrates superior collagen-stimulating potential with minimal inflammation compared to other PLA isomers.
Clinically, PLLA is used for facial volumization, wrinkle reduction, and overall skin improvement. Its degradation occurs via hydrolytic scission through a bulk erosion mechanism, with by-products consisting of lactic acid, a natural metabolic waste product the human body already produces. This renders PLLA extremely biocompatible. A study by Suuronen found that PLLA implanted in sheep maintained its macroscopic structure even after 5 years. The average duration of clinical effect is 18-24 months, with collagen stimulation continuing for up to 2 years. PLLA is available in lyophilized powder form requiring reconstitution before use, with examples including Sculptra and Olidia.
PDLLA: The Amorphous Alternative
PDLLA (Poly-DL-lactic acid), also known as poly(D,L-lactide), is an amorphous polymer made from a racemic mixture of L- and D-lactide monomers. Its random arrangement on the polymer backbone interferes with chain packing, resulting in no melting temperature and a lower glass transition temperature (Tg ≈ 55°C). This amorphous structure makes PDLLA more susceptible to degradation, with a typical degradation time of 12-16 months, compared to 24+ months for PLLA.
According to Harley Academy's guide, PDLLA "offers a balance between PLLA and PDLA properties, potentially providing a good balance of collagen stimulation and inflammation response". It is emerging as a promising treatment option in facial aesthetics. PDLLA shows variable inflammatory responses and collagen regeneration capacities, making it suitable for patients who want to see results more quickly. PDLLA formulations such as Aesthefill and Juvelook are available in lyophilized powder form requiring reconstitution, with some newer products combining PDLLA with non-cross-linked HA for enhanced effects.
PDLA: The Less Common Option
PDLA (Poly-D-lactic acid) consists of all D-isomers of lactic acid. It is less studied in aesthetic medicine and is generally associated with more inflammation and less collagen stimulation compared to PLLA. According to the Harley Academy, PDLA is "not as commonly used in aesthetic medicine". Most research and clinical applications focus on PLLA and PDLLA, with PDLA playing a relatively minor role in aesthetic practice.
Clinical Comparison: PLLA vs. PDLLA
| Feature | PLLA | PDLLA |
|---|---|---|
| Molecular Structure | Semi-crystalline (all L-isomers) | Amorphous (L + D isomers) |
| Melting Temperature | 170-200°C | None (amorphous) |
| Degradation Time | 24+ months | 12-16 months |
| Collagen Stimulation | Superior with minimal inflammation | Good balance, variable response |
| Injection Form | Lyophilized powder (reconstitution) | Lyophilized powder (reconstitution) |
| Typical Products | Sculptra, Olidia | Aesthefill, Juvelook |
| Clinical Application | Volume restoration, deep wrinkles | Faster results, skin quality, superficial concerns |
Clinical Applications and Patient Selection
The choice between PLLA and PDLLA should be guided by patient goals, timeline, and skin condition. According to a comprehensive review, PLLA is suitable for "facial overall rejuvenation, facial contouring, improving skin laxity and fine lines, and treating large areas of volume loss such as cheeks and temples". The ideal patient is typically 25-45 years old seeking gradual, natural-looking improvement with results appearing at 1-3 months and stabilizing at 3-6 months. PDLLA, with its faster degradation, is better suited for patients who want quicker results and skin quality enhancement on the neck and hands.
A 2025 expert guideline published in the Journal of Cosmetic Dermatology notes that "there are currently two distinct varieties of PLA-based fillers available on the market: PLLA and PDLLA. Both materials have been widely utilized in the field of aesthetic dermatology, primarily due to their capacity to induce a sub-clinical inflammatory tissue response that causes an increase in the content of type I collagen at the injection site". However, practitioners should be aware that PDLLA nodules, unlike HA nodules, do not respond to hyaluronidase treatment and require more intensive management.
Safety Profiles and Considerations
The 2025 expert guideline on PDLLA nodules emphasizes the importance of recognizing potential complications. While PDLLA has demonstrated a favorable safety profile, "although side effects are typically mild and transient, there are rare reports of more significant issues, such as nodules or granulomas". Unlike hyaluronic acid nodules that can be dissolved with hyaluronidase, PDLLA nodules "do not respond to straightforward enzymatic treatment, requiring a more intensive approach".
The management of these nodules requires accurate diagnosis and appropriate treatment based on the type (inflammatory or non-inflammatory) and onset timing. Strategies include vigorous massage, ultrasound-guided intervention, and in some cases, energy-based devices that leverage PDLLA's lower glass transition temperature for non-invasive reshaping. A structured diagnostic and treatment flowchart has been proposed to guide clinical management. For practitioners seeking high-quality biostimulatory fillers for their practice, Aurothread's PLLA filler collection offers clinically validated products with documented safety profiles.
Conclusion
Understanding the differences between PLLA, PDLLA, and PLA is essential for optimal treatment outcomes in aesthetic medicine. PLLA remains the gold standard for gradual, long-lasting volume restoration and collagen stimulation due to its superior collagen-stimulating potential and minimal inflammation. PDLLA provides a faster-degrading alternative with good collagen stimulation but requires careful nodule management. PDLA and other PLA variants are less common in aesthetic practice.
The 2026 SPAR review confirms that PLLA demonstrates superior collagen-stimulating potential with minimal inflammation, while PDLA and PDLLA exhibit variable inflammatory responses. By matching the right biostimulator to the patient's clinical goals and skin condition, practitioners can achieve natural-looking, long-lasting results with minimal complications.