
CaHA vs PLLA Fillers: Definitive Clinical Comparison 2026
Choosing between Calcium Hydroxylapatite (CaHA) and Poly-L-Lactic Acid (PLLA) fillers represents a critical clinical decision in aesthetic medicine. These two biostimulators are not interchangeable – each has unique material properties, clinical timelines, safety profiles, and optimal indications. CaHA, best known as Radiesse, provides immediate structural support through mineral-like microspheres in a carboxymethylcellulose gel carrier. PLLA, widely recognized as Sculptra, works gradually by stimulating fibroblasts to produce new collagen over several months. According to a 2023 survey by the American Society of Plastic Surgeons (ASPS) , 72% of aesthetic clinics now offer both biostimulator types, using patient-specific factors to guide selection. This definitive clinical comparison draws on evidence from the FDA, American Academy of Dermatology (AAD) , International Society of Aesthetic Plastic Surgery (ISAPS) , and peer-reviewed literature. For practitioners seeking high-quality products, both Aurothread's PLLA filler collection and CAHA product line offer clinically validated options with documented safety profiles.
Mechanism and Clinical Timeline Differences
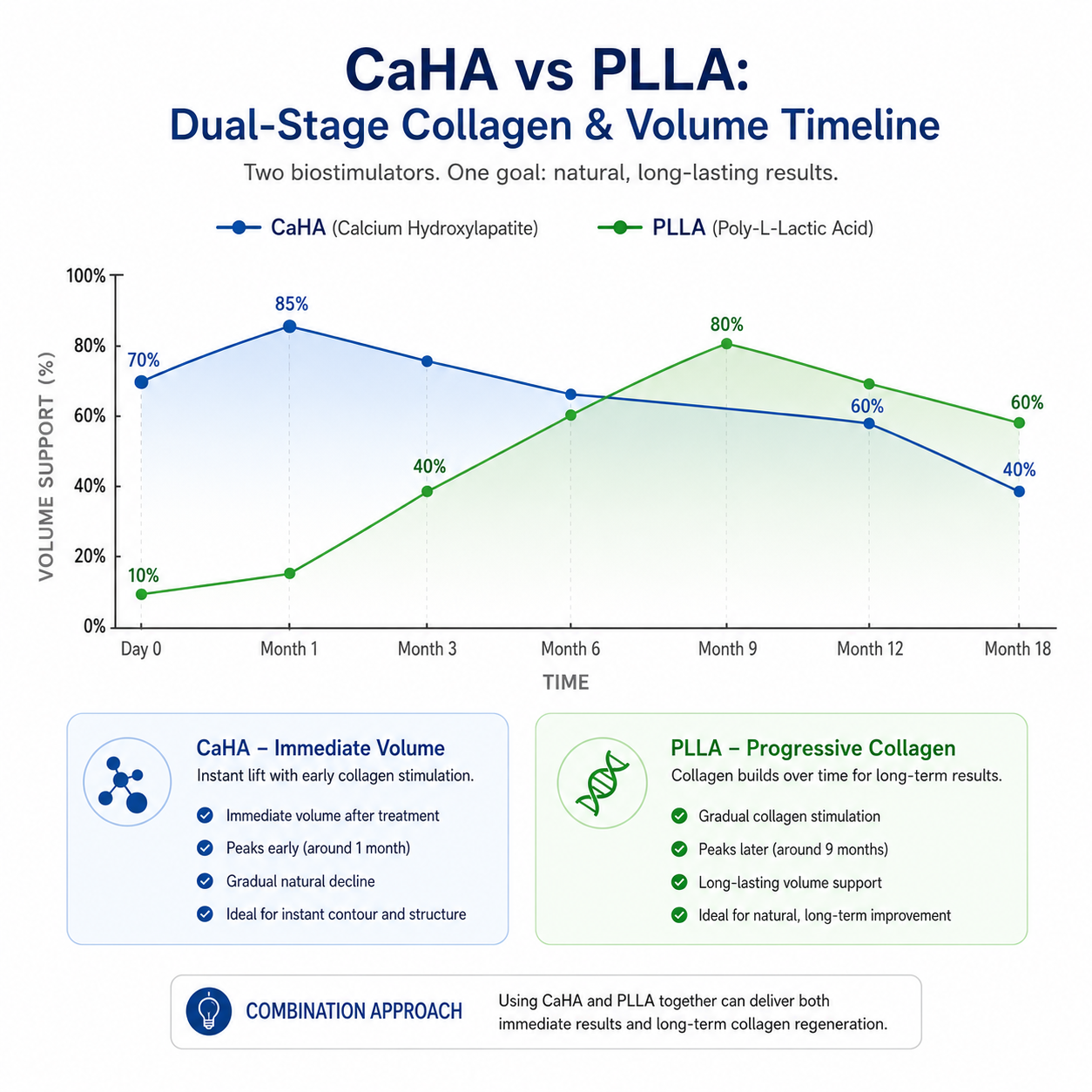
The biological mechanism of CaHA and PLLA differs fundamentally, directly impacting patient counseling. CaHA filler contains 25-45μm smooth microspheres of calcium hydroxylapatite – a mineral identical to human bone – suspended 1:1 in a CMC gel carrier. The gel provides immediate volume upon injection, while the particles act as a scaffold for Type I and Type III collagen deposition. A 2021 histological study in the Journal of Biomedical Materials Research found that CaHA increased collagen density by 210% at 6 months. According to FDA labeling, CaHA is indicated for deep dermal and subdermal injection for correction of moderate to severe facial wrinkles and folds, as well as hand augmentation. The visible result evolves from immediate scaffolding (gel) to long-term biological integration (particles), with most patients seeing peak aesthetic effect at 3-4 months.
PLLA follows a completely different pathway. This synthetic, biodegradable polymer (derived from corn starch) is supplied as lyophilized powder requiring reconstitution 2-24 hours before use. PLLA particles are larger (40-63μm) and irregularly shaped. When injected, they initiate a controlled inflammatory response where macrophages engulf particles and release cytokines that activate fibroblasts. Unlike CaHA, PLLA provides no immediate volume – in fact, patients may appear subjectively worse in the first week due to swelling. A 2022 study in Plastic and Reconstructive Surgery tracking 80 PLLA patients using 3D volumetric imaging found facial volume restoration of only 12% at week 2, 38% at week 12, and peak 72% at week 24. The AAD 2024 consensus statement emphasizes that PLLA requires 2-4 sessions spaced 4-6 weeks apart, with results emerging over 6-9 months and lasting 18-24 months.
For clinics, these timeline differences dictate follow-up scheduling. CaHA patients benefit from a 2-week "touch base" to see early results and a 6-month assessment for collagen-mediated improvement. PLLA patients require structured series documentation with photography at each session to demonstrate subtle changes. The reference article from MedWholesaleSupplies' CaHA vs PLLA comparison notes that patient satisfaction with PLLA was 89% when timeline counseling was thorough, versus 63% when patients were unprepared for delayed results.
Anatomic Indications and Injection Technique
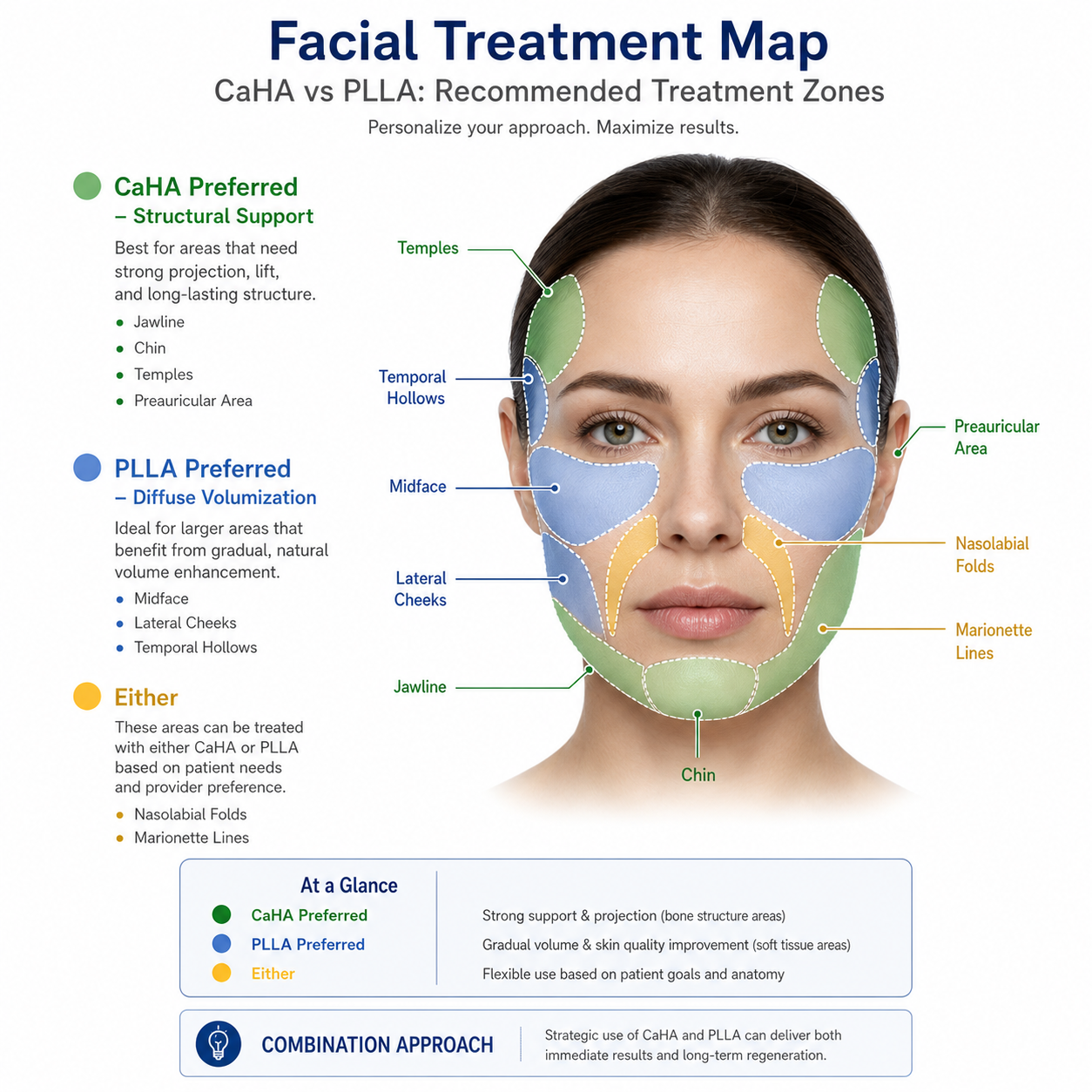
Anatomic site selection critically influences biostimulator choice. CaHA excels in areas requiring structural support and definition because its firm consistency resists deformation. According to ISAPS 2024 guidelines, CaHA is particularly appropriate for jawline contouring, chin augmentation, preauricular hollows, and temple volumization. A 2021 ultrasound study confirmed that CaHA injected at the periosteal level (directly on bone) provides the most predictable contour improvement, with 78% of patients maintaining definition at 12 months. However, CaHA is not recommended for dynamic areas like the lips or periocular region where stiffness could cause palpable nodules or unnatural movement. The injection technique uses small boluses (0.05-0.2mL) via 25G-27G needle or blunt cannula, followed by firm molding. The Aurothread CAHA collection offers products suitable for these structural applications.
PLLA is preferred for diffuse, generalized volume loss where the goal is gradual tissue thickening rather than sharp definition. The midface (malar region), lateral cheek hollows, and temporal concavities respond exceptionally well to PLLA. A 2020 randomized controlled trial found that PLLA-treated patients had a mean increase in dermal thickness of 4.2mm on ultrasound. Unlike CaHA, PLLA can be injected into more superficial planes (deep dermis to superficial subcutaneous) using a fanning or linear retrograde technique with a 25G-27G cannula. The key principle is even distribution – never inject PLLA as a bolus, as concentrated particle depots create high nodule risk. A single entry point may allow 5-10 fanning passes covering a large surface area. Aurothread's PLLA filler collection includes products specifically formulated for smooth extrusion during fanning techniques.
For hands, CaHA has a specific FDA indication and has been shown in a 2019 study to increase dorsal hand volume by 3.1mL per hand on average, with results lasting 12-15 months. PLLA has off-label hand use but requires more sessions and produces more subtle results. Temple augmentation demands particular caution with both products due to the superficial temporal artery. The reference article emphasizes verifying current product indication, approved anatomic area, and scope requirements before building protocols.
Safety Profiles and Adverse Event Management
Both biostimulators have favorable safety profiles when used by trained practitioners, but adverse event patterns differ substantially. According to a 2023 systematic review in JAMA Dermatology analyzing 25,000 patients, the overall complication rate was 4.2% for CaHA and 5.8% for PLLA. For CaHA, immediate events include injection-site swelling (45-60%, lasting 2-7 days) and bruising (20-30%). Delayed visible nodules occur in 2.1% of patients, usually appearing 2-6 months post-injection. CaHA nodules are typically firm, round, and located at injection sites. Management includes observation, massage, or intralesional triamcinolone (2.5-5mg/mL). Critically, CaHA cannot be dissolved with hyaluronidase – a key counseling point. The FDA emphasizes that practitioners must be trained to recognize and manage vascular occlusion, which occurs in approximately 0.01% of CaHA cases and requires immediate recognition (blanching, pain), nitropaste application, and hyperbaric oxygen if available.
PLLA's adverse event profile is dominated by delayed inflammatory nodules. A 2020 pooled analysis of 2,100 PLLA patients found an overall nodule incidence of 6.8%, with 4.2% palpable only, 2.1% visible but not tender, and 0.5% visible and tender. These nodules typically appear 3-12 months post-treatment, caused by macrophage aggregation around PLLA particles. Management follows a stepwise approach: massage for non-tender nodules; intralesional 5-fluorouracil + triamcinolone (0.1mL of 50mg/mL 5-FU + 0.4mL of 10mg/mL triamcinolone) for persistent or tender nodules; and surgical excision for refractory cases (less than 0.1% incidence). According to FDA post-marketing surveillance, severe complications from PLLA are rare when proper reconstitution (minimum 2 hours hydration, ideally 24 hours) and injection technique are followed.
The reference MedWholesaleSupplies clinical comparison emphasizes that both products require clear consent language covering delayed lumps, asymmetry, and escalation instructions. Sudden severe pain, skin color change, or visual symptoms require urgent assessment – front-desk staff should not attempt diagnosis. For comprehensive safety protocols, consult the American Society for Dermatologic Surgery guidelines.
Reconstitution, Workflow, and Economic Considerations
Clinic workflow logistics differ substantially between these biostimulators. CaHA arrives as a sterile, ready-to-use suspension requiring no reconstitution – simply remove from packaging, attach a sterile needle (typically 25G-27G), and inject. Total preparation time: less than 60 seconds. Acquisition costs range from $400-600 per 1.5mL syringe, with clinics charging $800-1200 per session. Most patients achieve desired results with 1-2 syringes in a single session. The high per-session price appeals to patients seeking immediate, dramatic results with minimal time commitment. The Aurothread CAHA line offers ready-to-use syringes with documented sterility and particle size consistency.
PLLA requires significant preparation that impacts scheduling and staffing. The lyophilized powder (typically 150mg per vial) must be reconstituted with 5-8mL sterile water for injection, then hydrated for a minimum of 2 hours – though experts recommend 24 hours for optimal particle dispersion. A 2021 study in Dermatologic Surgery found that 24-hour hydration reduced clumping and injection resistance by 43% compared to 2-hour hydration. After hydration, 1-2mL of preservative-free lidocaine is added. The product must be swirled (never shaken) immediately before drawing into syringes. Improper preparation significantly increases nodule risk: inadequate hydration (less than 2 hours) caused palpable nodules in 14% of patients versus 2% when hydration exceeded 6 hours.
Economically, PLLA vials cost $150-250 each, with most patients requiring 2-4 sessions (typically 3 sessions spaced 6 weeks apart) using 1-2 vials per session. Total product cost per patient course ranges from $450-2000. Clinics charge $600-1000 per session, making total patient investment $1800-4000. While per-session margins are similar to CaHA (50-60%), the longer treatment course generates higher total revenue but requires greater patient commitment and clinic visit capacity. The reference article notes that practices must build a small formulary to reduce variability across injectors, with documented lot traceability, expiration dates, and storage conditions.
Conclusion: Matching Biostimulator to Patient Goals
CaHA and PLLA are both excellent biostimulators, but their optimal applications are distinct. CaHA is the preferred choice for patients seeking immediate, structural correction of focal volume deficits – sharp jawlines, defined chins, projected cheekbones, and hand rejuvenation. Its advantages include single-session treatment, visible results within days, and no reconstitution requirements. However, CaHA cannot be dissolved, carries a small risk of visible nodules (2.1%), and provides structural rather than diffuse volumization.
PLLA is ideal for patients with diffuse, age-related volume loss who accept a gradual timeline. Its advantages include natural, progressive results over 6-9 months, broader tissue coverage, and documented collagen stimulation lasting 18-24 months. The trade-offs are significant: 2-4 treatment sessions, 6-12 months to final results, reconstitution complexity (2-24 hours preparation), and higher nodule incidence (6.8% overall, though most are palpable only).
For clinics building their biostimulator formulary, carrying both products enables optimal patient matching. The reference MedWholesaleSupplies comparison concludes that the right choice depends on indication, anatomy, patient history, training, and follow-up capacity. For high-quality, clinically validated products, Aurothread's PLLA filler collection and CAHA product line provide sterile, traceable options with documented manufacturing standards. Always combine product selection with hands-on training, clear consent, and disciplined follow-up – the key to successful biostimulator outcomes.
Choosing the right biostimulator starts with a trusted partner. Contact Aurothread now for expert guidance on CaHA, PLLA, and all your dermal filler needs.